Primer on Cardiac Surgery for General Surgery Residents
By Lambros Tsonis MD
Introduction
Welcome to your cardiothoracic surgery rotation. We, the cardiac surgery faculty, hope that this rotation will expose you to the enormous complexity of surgery in the chest. While your focus on this rotation will be on non-cardiac thoracic surgery, opportunities to participate in cardiac procedures will likely present themselves during your rotation, and this document is intended as a primer to familiarize you to cardiac surgery and thoracic procedures which require the use of cardiopulmonary bypass. This document is not meant to be all-encompassing, and is intended to be more of a summary. There are myriads of other resources that are more in-depth that are available to you if you would like to learn more about a topic.
As the PGY-4 resident on thoracic surgery, your responsibilities regarding the cardiac surgery patients are limited to covering those patients and cases when you are on call. During weekdays, if you are contacted regarding issues with a cardiac surgery patient, please refer the caller to the fellows or NPs covering the cardiac patients. When you are on call, you are covering the fellow's call responsibilities, and will be required to participate in cases or evaluate the patients as the fellows would. This primer will help give you some of the requisite information to do that. As always, if you have any questions or are unsure what the best course of action is, feel free to contact the appropriate attending directly. All of us are easily approachable and would rather answer a phone call from you than deal with a less than ideal patient outcome.
Emergent Cardiac Consultations
If called to see a cardiac surgery consultation, it is important to differentiate emergent conditions from those that are not emergencies. A few questions to ask when you get the call:
For emergent consults, focus your history on the problem. When did the chest pain (or angina equivalent) start? Have you had similar symptoms before? Any associated dyspnea/syncope/dizziness? Any prior coronary interventions/stents/CABG? Is the patient on any blood thinners/anticoagulants? Any history of CVA/renal disease/liver disease? What workup has been done so far?
For cardiac consults, the patients generally have had an echocardiogram and a cardiac cath before we are called. You are not expected to be able to read an echo, but a reasonable question to ask is what is the ejection fraction? Are there any wall motion abnormalities? Is there any severe valvular pathology? Is there any fluid around the heart? Similarly, you may not be able to interpret a cardiac cath, but you should know that most patients have a left main (LM) and a right coronary artery (RCA). The LM quickly bifurcates in most patients to the left anterior descending (LAD) and left circumflex (LCx) arteries. If the LAD, RCA, and LCx all have some significant disease, this is commonly referred to as 3-vessel disease. Other branches of these vessels exist, and some are named, but if you just know these arteries you will know a lot. Of the arteries mentioned, the LAD is the most important; it supplies about 50-60% of the blood to the heart. Stenoses greater than 50% may be significant; acute occlusion implies an MI is happening. If the cardiologists are calling us emergently from the cath lab for an acute MI, it generally means one of a few things:
Aortic dissections
Another emergent condition that you will be called about with some frequency is an aortic dissection. Aortic dissections are partial thickness tears of the aortic wall such that blood travels in the media as well as in the true lumen. They can be differentiated into 2 broad types by the Stanford classification. Type A dissections originate in or involve the ascending aorta. These are surgical emergencies that need to go to the OR ASAP. Any dissection that begins beyond the pericardial reflection (arch or distal) is a Type B. Type B dissections can generally be managed medically with aggressive blood pressure control, provided there is no malperfusion. In both cases, always ask if the CT was done with IV contrast. A non-contrast CT cannot definitively diagnose an aortic dissection. Also, ask what was scanned. Frequently they will get an abdominal CT that showed a dissection and no imaging of the chest. In evaluating any aortic dissection, you must visualize the ascending aorta with a contrasted study. If you are called to see any type A dissection, call the attending early.
Some more background on aortic dissections can be found in video format here.
ECMO evaluations
Another reason for an urgent/emergent consultation is for ECMO (extracorporeal membrane oxygenation) support. There are 2 basic reasons why someone may need ECMO: either respiratory failure or cardiogenic shock. We have a busy lung transplant program at Loyola, and we are frequently called to see patients with end stage pulmonary failure who are either listed for transplant or are being evaluated for listing and have respiratory failure. In these cases, see the patient expeditiously. Ask if an ABG has been done recently (frequently it hasn't; if not, get one). Find out what central lines they have, and how much oxygen they are on. We try not to intubate these patients, as they have a tendency to decompensate with intubation. Generally these patients are supported with veno-venous ECMO (VV ECMO) to oxygenate their blood and clear CO2 while we wait for lungs to become available for transplantation. This can also be used as a bridge to recovery of the patient's native lungs (such as with COVID-19 or H1N1 influenza).
With cardiogenic shock (which may or may not also be associated with respiratory failure), the heart's cardiac output is not sufficient to maintain organ perfusion to the body. This may be caused by an MI, cardiomyopathy, toxin, or something else. These patients generally require veno-arterial ECMO (VA ECMO) for support, either temporarily as a bridge to recovery, or as a bridge to either LVAD or heart transplant.
Non-emergent Cardiac Consultations
While on call, you may be asked to evaluate patients with cardiac disease for cardiac surgery. In these stable patients, a detailed H&P is always a good start. You will have the opportunity to review the patient's imaging and discuss with the attending in a more orderly fashion. If you are called for one of these consults, and you have already left the hospital, they can generally be seen on the morning. If you are unsure, you can ask the cardiologist (who is calling you) if the patient needs to be seen now or if it can wait until the next morning. Typical indications for non-emergent cardiac surgery evaluations include:
Preoperative Assessment
In general, most patients will have already had an extensive workup done by the medical services before we are called. You should review all the available data before seeing the patient. If the patient had imaging from an outside hospital, please make sure those images are uploaded to LifeImage and seen by the attending. When seeing the patient, in addition to all the normal things you would review with a good H&P, you should note the following:
Surgical Considerations
All cardiac surgery patients, when they come to the OR, will need invasive monitoring and good IV access. This is generally accomplished with a Cordis and Swan-Ganz catheter and an arterial line. If you are unfamiliar with Swan-Ganz catheters, it would be a good idea to review the course of a Swan-Ganz catheter through the heart and the various pressure tracings seen during insertion prior to the start of the rotation. The patients are all intubated, and the EKG leads and defibrillator pad are placed on the back. Patients are positioned supine on the operating room table with both arms tucked at the side and a shoulder roll placed behind the upper shoulders. Patients have any body hair clipped from the chin to the ankles. The legs are slightly rotated externally and secured to the bed with tape and blankets. The standard surgical prep is to prep from the neck to the ankles. Most cardiac surgery operations are done via a median sternotomy incision. The exceptions to this include bilateral lung transplants (generally done through a clamshell incision; require the arms elevated over the patient's head), unilateral lung transplants (generally done through a thoracotomy with the hips flexed to allow for femoral access), descending thoracic/thoracoabdominal aneurysms (done through either a left thoracotomy or thoracoabdominal incision), and LVAD exchanges (done through a subcostal incision).
Once the patient has been prepped and draped, incisions will be made and the operation begins. The heart will be exposed by dividing the sternum and opening the pericardium. Most of what you can see without lifting the heart will be right ventricle, but right atrium, SVC, aorta, and pulmonary artery should all be visible. Depending on the operation being performed, conduit may be harvested at this point. Saphenous vein is usually harvested by the surgical assistants, while internal mammary artery or radial artery is usually harvested by the surgeons.
Once this is completed, preparations will be made to connect the patient to the cardiopulmonary bypass machine. This machine is essentially a pump that allows us to continue blood circulation while the heart is stopped. It is also connected to an oxygenator that allows for gas exchange and a heater/cooler that allows us to adjust the patient's body temperature. The cardiopulmonary bypass machine is managed by a perfusionist under the direction of the surgeon. To work, at least 2 cannulae have to be inserted in the patient: a venous cannula to drain blood out of the patient and send it to the machine, and an arterial cannula where blood can be returned to the patient. These cannulae are held in place by pursestring sutures placed before cannulating. Most commonly, we cannulate the right atrium for the venous cannula and the aorta for the arterial, but this can be different depending on the operation being performed. Prior to initiating cardiopulmonary bypass, the patient will be heparinized, and the perfusionist will be responsible for monitoring activated clotting times (ACTs) and re-dosing heparin as appropriate.
Myocardial protection
If the operation involves stopping the heart, then a strategy must be in place to protect the myocardium from ischemia. This is generally done by the administration of cardioplegia, which is a solution that is very cold (4oC) and hyperkalemic, which may be mixed with blood. The cardioplegia can be delivered antegrade by inserting a cannula into the ascending aorta, or retrograde by inserting a cannula into the right atrium and directing it into the coronary sinus. If the aorta is opened during the operation, cardioplegia can also be given directly into the coronary ostia. The hyperkalemic cardioplegia induces a flaccid paralysis of the heart, and the cold temperature reduces myocardial oxygen consumption. Cardioplegia will be given at regular intervals while the heart is arrested to attempt to minimize myocardial ischemia. Once the cardioplegia cannula(e) are inserted, the aorta is cross clamped, cardioplegia is given, and the heart is topically cooled with ice while the perfusionist systemically cools the patient. The degree to which the patient is cooled is variable, depending on the operation performed, from around 32oC for most CABGs to 18oC for cases requiring deep hypothermic circulatory arrest.
Procedure
Once the heart is stopped, the intended cardiac intervention can be performed. For CABG, this involves identifying the diseased coronary artery distal to the identified stenosis, creating an arteriotomy, and making an end-to-side anastomosis between the conduit and the coronary artery. Once the distal anastomosis is completed, a proximal anastomosis is constructed on the ascending aorta. It is beyond the scope of this primer to describe every cardiac operation, but this should be discussed with the attending and reviewed prior to scrubbing into the case.
Circulatory Arrest and Cerebral protection
For most aortic dissections, in order to do the distal anastomosis, there is not enough room to have a cross clamp and be able to sew a graft to the underside of the aortic arch. In these cases (and other cases where one needs to operate in a bloodless field), the patient needs deep hypothermic circulatory arrest. The patient is cooled to 18oC for at least 45 minutes. Then, the cardiopulmonary bypass machine is stopped and the cross clamp is removed. At this point, the only thing protecting the patient's brain and other organs from irreversible ischemia is severe hypothermia and the reduced oxygen consumption that induces. With the cross clamp now removed, the distal anastomosis involving the arch can be performed. Typically, we will pass antegrade cerebral perfusion catheters to deliver blood to the brain via the innominate and carotid arteries while under circulatory arrest. Using this technique, patients may safely undergo circulatory arrest for up to 60 minutes (though shorter is obviously better).
Weaning off cardiopulmonary bypass and closure
Once the intended procedure is completed, the patient will be given blood via the cardioplegia circuit to wash out the extra potassium from the heart and rewarm the heart. As this happens, the heart will generally start to beat. The cross clamp is then removed. The heart is then given time to recover from cardioplegia while circulation is supported by the pump, and inotropes/pressors are begun while the lungs are re-inflated. Once the heart is beating well, the patient is normothermic, and appropriate inotropes/pressors are working, the patient will be weaned off cardiopulmonary bypass by the surgeon. Once off bypass, the cannulas are removed and the pre-placed pursestring sutures will be tied. There is always some degree of coagulopathic bleeding at this point; this is managed by giving protamine and blood products. Temporary ventricular pacing wires are generally also placed, and, occasionally, atrial wires can also be placed. Typically, at least 2 chest tubes are placed to drain the mediastinum/left chest. Sternal closure is most often done with sternal wires, though other systems are sometimes used. Fascia, subcutaneous tissue, and skin is then closed. As you are closing, the nurse will connect the chest tubes to suction and look for blood accumulating in the tubing. This is referred to as “timing”. To pass timing, you will need to see that no blood is accumulating in the chest tubes after 5 minutes; this is done at least 3 times. This gives us a rudimentary assessment if bleeding is a concern before drapes are taken down and the patient is brought to the ICU.
You should stay with the patient as the patient is brought out of the OR and transferred to the ICU. As drips are disconnected/reconnected and the patient’s hemodynamic monitoring is transitioned, or as the patient is rolled/moved, patients can have significant hemodynamic changes and you should always be watching for these. Typically, it is a good idea to stay at the patient’s bedside in the ICU until all the monitors are hooked up, report has been given to the nurse and the ICU residents/attending, hemodynamics are stabilized, and you are satisfied that there isn’t major uncontrolled bleeding. If in doubt, notify the attending immediately.
A video outline of cardiopulmonary bypass can be found here.
Routine postoperative care
Postop cardiac surgery patients have a standard protocol that the nurses follow for routine care. This may not be appropriate in all patients; the attending will let you and the nurses know what he wants. Typically, if there is no significant bleeding over the next few hours postop, the pressors and inotropes will be slowly weaned off and the patient will be allowed to wake up, with the goal of extubating within 6 hours. Typically, on POD 1, the Swan-Ganz catheter is removed and the patient is ambulated. Beta blockers and diuretics are frequently begun. Aspirin, lovenox, and sometimes other anticoagulants are begun. Chest tubes are removed by the ICU nurses at the direction of the surgeon when the output is low (generally less than 200cc/day). By POD 2, central lines, foley, and chest tubes are generally out. Patients at this stage generally transfer to telemetry. The remainder of the postoperative course is working on pain control, ambulation, and medication adjustments for heart rate/blood pressure/diuretics/anticoagulation. The NPs on the floor will handle most of the routine orders and make arrangements for outpatient f/u, home health care services, etc. Typically, patients are ready for discharge home after uncomplicated cardiac surgery by POD 5.
Postoperative Complications
Generally speaking, you will not be called for the cardiac surgery patient that is doing well. The nurses and ICU residents will be calling you to help address problems. In dealing with any of these issues, if you have concerns or questions about what is the most appropriate treatment, contact the attending directly and ask. All of us will want to know early if there are postoperative issues with our patients. Some of the more common problems cardiac surgery patients encounter are listed below.
Bleeding/tamponade
As previously mentioned, there is always some degree of bleeding after heart surgery. Bleeding from coagulopathy can happen as clotting factors are consumed by the use of the cardiopulmonary bypass machine, heparin is given, or platelets don’t work due to medications the patient was on preoperatively. Obviously, not all bleeding is from coagulopathy, and evaluation in the OR to achieve adequate hemostasis is mandatory. Timing at the end of the case is useful to see if the bleeding is under control; if you are not making times, you should not leave the OR and you need to let the attending know. While 3x5min is a common method used, some attendings will use different metrics to assess for bleeding; they will let you know what they want. Once the patient is brought to the ICU, it is a good idea to record the level of the chest tube output (frequently there is a dump of blood as the patient is being jostled and moved). If there is a concern for bleeding in the ICU, make sure to keep the chest tubes patent by stripping the chest tubes; this is done by applying lotion or other lubrication to the soft part of the tubing and pulling it backwards, creating a suction in the chest tube and allowing clots to be pulled backwards. Keep an eye on the chest tube output at 15 minute intervals initially. Generally, output >100cc/hr is too much. Blood products, K centra, protamine, or Factor VII may all be given, but, if this persists, the patient may need to return to the OR.
In managing a bleeding patient with the chest closed in the ICU, you must be aware of the possibility of tamponade, even if the chest tubes are patent and working. Look for hypotension unresponsive to pressors, a reduction of cardiac output as measured by the Swan-Ganz catheter, and an equalization of the CVP and the PA diastolic pressure. To help make the diagnosis, a chest x-ray may be helpful to look for a widened mediastinum. You can also request either a bedside transthoracic echo (done by the cardiology fellow) or a transesophageal echo (done by cardiac anesthesia) to look for fluid around the heart and see if that fluid is collapsing the RV in diastole. If you are worried about tamponade in any patient, call the attending immediately.
There are extreme cases where there is tamponade in a patient in the ICU and there is no time to bring the patient to the OR. You should be discussing these situations with the attending, and you may be directed to open the chest in a patient in the ICU. This is only to be done at the explicit instruction of the CV surgery attending. There is a cart in the ICU that has the instruments you would need for this: a sterile drape to drape the chest, a scalpel to reopen the skin and cut the sutures for the subcutaneous and fascial closures, a heavy twister to partially untwist the sternal wires, a wire cutter to cut the sternal wires, and a sternal retractor to open the sternum. There is also suction tubing to connect to wall suction. Once the sternum is opened, the patient’s hemodynamics should immediately improve. If you see a bleeding source squirting at you, put your finger on it; otherwise, suction the blood and wait for the attending.
An informative video summary of this subject can be found here.
By Lambros Tsonis MD
Introduction
Welcome to your cardiothoracic surgery rotation. We, the cardiac surgery faculty, hope that this rotation will expose you to the enormous complexity of surgery in the chest. While your focus on this rotation will be on non-cardiac thoracic surgery, opportunities to participate in cardiac procedures will likely present themselves during your rotation, and this document is intended as a primer to familiarize you to cardiac surgery and thoracic procedures which require the use of cardiopulmonary bypass. This document is not meant to be all-encompassing, and is intended to be more of a summary. There are myriads of other resources that are more in-depth that are available to you if you would like to learn more about a topic.
As the PGY-4 resident on thoracic surgery, your responsibilities regarding the cardiac surgery patients are limited to covering those patients and cases when you are on call. During weekdays, if you are contacted regarding issues with a cardiac surgery patient, please refer the caller to the fellows or NPs covering the cardiac patients. When you are on call, you are covering the fellow's call responsibilities, and will be required to participate in cases or evaluate the patients as the fellows would. This primer will help give you some of the requisite information to do that. As always, if you have any questions or are unsure what the best course of action is, feel free to contact the appropriate attending directly. All of us are easily approachable and would rather answer a phone call from you than deal with a less than ideal patient outcome.
Emergent Cardiac Consultations
If called to see a cardiac surgery consultation, it is important to differentiate emergent conditions from those that are not emergencies. A few questions to ask when you get the call:
- Is the patient hemodynamically stable?
- Is the patient having active chest pain?
- What is the patient's respiratory status?
- What does the patient's EKG look like?
For emergent consults, focus your history on the problem. When did the chest pain (or angina equivalent) start? Have you had similar symptoms before? Any associated dyspnea/syncope/dizziness? Any prior coronary interventions/stents/CABG? Is the patient on any blood thinners/anticoagulants? Any history of CVA/renal disease/liver disease? What workup has been done so far?
For cardiac consults, the patients generally have had an echocardiogram and a cardiac cath before we are called. You are not expected to be able to read an echo, but a reasonable question to ask is what is the ejection fraction? Are there any wall motion abnormalities? Is there any severe valvular pathology? Is there any fluid around the heart? Similarly, you may not be able to interpret a cardiac cath, but you should know that most patients have a left main (LM) and a right coronary artery (RCA). The LM quickly bifurcates in most patients to the left anterior descending (LAD) and left circumflex (LCx) arteries. If the LAD, RCA, and LCx all have some significant disease, this is commonly referred to as 3-vessel disease. Other branches of these vessels exist, and some are named, but if you just know these arteries you will know a lot. Of the arteries mentioned, the LAD is the most important; it supplies about 50-60% of the blood to the heart. Stenoses greater than 50% may be significant; acute occlusion implies an MI is happening. If the cardiologists are calling us emergently from the cath lab for an acute MI, it generally means one of a few things:
- They can't cross the culprit lesion with a wire or stent and the patient needs emergent CABG.
- They dissected/perforated/occluded a coronary artery
- They treated the lesion, but the patient has cardiogenic shock and may need ECMO
- The critical lesion is in the distal left main (these patients need emergent CABG)
Aortic dissections
Another emergent condition that you will be called about with some frequency is an aortic dissection. Aortic dissections are partial thickness tears of the aortic wall such that blood travels in the media as well as in the true lumen. They can be differentiated into 2 broad types by the Stanford classification. Type A dissections originate in or involve the ascending aorta. These are surgical emergencies that need to go to the OR ASAP. Any dissection that begins beyond the pericardial reflection (arch or distal) is a Type B. Type B dissections can generally be managed medically with aggressive blood pressure control, provided there is no malperfusion. In both cases, always ask if the CT was done with IV contrast. A non-contrast CT cannot definitively diagnose an aortic dissection. Also, ask what was scanned. Frequently they will get an abdominal CT that showed a dissection and no imaging of the chest. In evaluating any aortic dissection, you must visualize the ascending aorta with a contrasted study. If you are called to see any type A dissection, call the attending early.
Some more background on aortic dissections can be found in video format here.
ECMO evaluations
Another reason for an urgent/emergent consultation is for ECMO (extracorporeal membrane oxygenation) support. There are 2 basic reasons why someone may need ECMO: either respiratory failure or cardiogenic shock. We have a busy lung transplant program at Loyola, and we are frequently called to see patients with end stage pulmonary failure who are either listed for transplant or are being evaluated for listing and have respiratory failure. In these cases, see the patient expeditiously. Ask if an ABG has been done recently (frequently it hasn't; if not, get one). Find out what central lines they have, and how much oxygen they are on. We try not to intubate these patients, as they have a tendency to decompensate with intubation. Generally these patients are supported with veno-venous ECMO (VV ECMO) to oxygenate their blood and clear CO2 while we wait for lungs to become available for transplantation. This can also be used as a bridge to recovery of the patient's native lungs (such as with COVID-19 or H1N1 influenza).
With cardiogenic shock (which may or may not also be associated with respiratory failure), the heart's cardiac output is not sufficient to maintain organ perfusion to the body. This may be caused by an MI, cardiomyopathy, toxin, or something else. These patients generally require veno-arterial ECMO (VA ECMO) for support, either temporarily as a bridge to recovery, or as a bridge to either LVAD or heart transplant.
Non-emergent Cardiac Consultations
While on call, you may be asked to evaluate patients with cardiac disease for cardiac surgery. In these stable patients, a detailed H&P is always a good start. You will have the opportunity to review the patient's imaging and discuss with the attending in a more orderly fashion. If you are called for one of these consults, and you have already left the hospital, they can generally be seen on the morning. If you are unsure, you can ask the cardiologist (who is calling you) if the patient needs to be seen now or if it can wait until the next morning. Typical indications for non-emergent cardiac surgery evaluations include:
- 3 vessel coronary disease
- Left main disease
- Coronary disease not able to be stented
- Severe valvular heart disease, with or without concomitant coronary disease
- Endocarditis
- End stage heart failure/referral for heart transplant or LVAD
- Lung transplant evaluations
- Type B dissections
- Ascending/arch/descending thoracic aortic aneurysms
Preoperative Assessment
In general, most patients will have already had an extensive workup done by the medical services before we are called. You should review all the available data before seeing the patient. If the patient had imaging from an outside hospital, please make sure those images are uploaded to LifeImage and seen by the attending. When seeing the patient, in addition to all the normal things you would review with a good H&P, you should note the following:
- Has the patient had prior heart surgery or stenting?
- Has the patient had saphenous vein stripping or vein harvested for other procedures (such as for peripheral vascular disease)?
- Does the patient have loose teeth/poor dentition?
- Is the patient on anticoagulant medication? If so, what is the indication for anticoagulation and can the medication be stopped?
- Is the patient a current smoker? If so, are they interested in quitting?
- Is the patient an alcoholic or a drug abuser?
- Does that patient appear robust/reasonably healthy such that they can tolerate a cardiac surgery? What sort of activity does the patient do on a regular basis?
- Full set of labs (CBC, CMP, coags, type and cross 4 units)
- Recent chest X-ray
- EKG
- Echocardiogram
- Cardiac cath
- Carotid evaluation (duplex or CTA or MRA)
- PFTs or spirometry
Surgical Considerations
All cardiac surgery patients, when they come to the OR, will need invasive monitoring and good IV access. This is generally accomplished with a Cordis and Swan-Ganz catheter and an arterial line. If you are unfamiliar with Swan-Ganz catheters, it would be a good idea to review the course of a Swan-Ganz catheter through the heart and the various pressure tracings seen during insertion prior to the start of the rotation. The patients are all intubated, and the EKG leads and defibrillator pad are placed on the back. Patients are positioned supine on the operating room table with both arms tucked at the side and a shoulder roll placed behind the upper shoulders. Patients have any body hair clipped from the chin to the ankles. The legs are slightly rotated externally and secured to the bed with tape and blankets. The standard surgical prep is to prep from the neck to the ankles. Most cardiac surgery operations are done via a median sternotomy incision. The exceptions to this include bilateral lung transplants (generally done through a clamshell incision; require the arms elevated over the patient's head), unilateral lung transplants (generally done through a thoracotomy with the hips flexed to allow for femoral access), descending thoracic/thoracoabdominal aneurysms (done through either a left thoracotomy or thoracoabdominal incision), and LVAD exchanges (done through a subcostal incision).
Once the patient has been prepped and draped, incisions will be made and the operation begins. The heart will be exposed by dividing the sternum and opening the pericardium. Most of what you can see without lifting the heart will be right ventricle, but right atrium, SVC, aorta, and pulmonary artery should all be visible. Depending on the operation being performed, conduit may be harvested at this point. Saphenous vein is usually harvested by the surgical assistants, while internal mammary artery or radial artery is usually harvested by the surgeons.
Once this is completed, preparations will be made to connect the patient to the cardiopulmonary bypass machine. This machine is essentially a pump that allows us to continue blood circulation while the heart is stopped. It is also connected to an oxygenator that allows for gas exchange and a heater/cooler that allows us to adjust the patient's body temperature. The cardiopulmonary bypass machine is managed by a perfusionist under the direction of the surgeon. To work, at least 2 cannulae have to be inserted in the patient: a venous cannula to drain blood out of the patient and send it to the machine, and an arterial cannula where blood can be returned to the patient. These cannulae are held in place by pursestring sutures placed before cannulating. Most commonly, we cannulate the right atrium for the venous cannula and the aorta for the arterial, but this can be different depending on the operation being performed. Prior to initiating cardiopulmonary bypass, the patient will be heparinized, and the perfusionist will be responsible for monitoring activated clotting times (ACTs) and re-dosing heparin as appropriate.
Myocardial protection
If the operation involves stopping the heart, then a strategy must be in place to protect the myocardium from ischemia. This is generally done by the administration of cardioplegia, which is a solution that is very cold (4oC) and hyperkalemic, which may be mixed with blood. The cardioplegia can be delivered antegrade by inserting a cannula into the ascending aorta, or retrograde by inserting a cannula into the right atrium and directing it into the coronary sinus. If the aorta is opened during the operation, cardioplegia can also be given directly into the coronary ostia. The hyperkalemic cardioplegia induces a flaccid paralysis of the heart, and the cold temperature reduces myocardial oxygen consumption. Cardioplegia will be given at regular intervals while the heart is arrested to attempt to minimize myocardial ischemia. Once the cardioplegia cannula(e) are inserted, the aorta is cross clamped, cardioplegia is given, and the heart is topically cooled with ice while the perfusionist systemically cools the patient. The degree to which the patient is cooled is variable, depending on the operation performed, from around 32oC for most CABGs to 18oC for cases requiring deep hypothermic circulatory arrest.
Procedure
Once the heart is stopped, the intended cardiac intervention can be performed. For CABG, this involves identifying the diseased coronary artery distal to the identified stenosis, creating an arteriotomy, and making an end-to-side anastomosis between the conduit and the coronary artery. Once the distal anastomosis is completed, a proximal anastomosis is constructed on the ascending aorta. It is beyond the scope of this primer to describe every cardiac operation, but this should be discussed with the attending and reviewed prior to scrubbing into the case.
Circulatory Arrest and Cerebral protection
For most aortic dissections, in order to do the distal anastomosis, there is not enough room to have a cross clamp and be able to sew a graft to the underside of the aortic arch. In these cases (and other cases where one needs to operate in a bloodless field), the patient needs deep hypothermic circulatory arrest. The patient is cooled to 18oC for at least 45 minutes. Then, the cardiopulmonary bypass machine is stopped and the cross clamp is removed. At this point, the only thing protecting the patient's brain and other organs from irreversible ischemia is severe hypothermia and the reduced oxygen consumption that induces. With the cross clamp now removed, the distal anastomosis involving the arch can be performed. Typically, we will pass antegrade cerebral perfusion catheters to deliver blood to the brain via the innominate and carotid arteries while under circulatory arrest. Using this technique, patients may safely undergo circulatory arrest for up to 60 minutes (though shorter is obviously better).
Weaning off cardiopulmonary bypass and closure
Once the intended procedure is completed, the patient will be given blood via the cardioplegia circuit to wash out the extra potassium from the heart and rewarm the heart. As this happens, the heart will generally start to beat. The cross clamp is then removed. The heart is then given time to recover from cardioplegia while circulation is supported by the pump, and inotropes/pressors are begun while the lungs are re-inflated. Once the heart is beating well, the patient is normothermic, and appropriate inotropes/pressors are working, the patient will be weaned off cardiopulmonary bypass by the surgeon. Once off bypass, the cannulas are removed and the pre-placed pursestring sutures will be tied. There is always some degree of coagulopathic bleeding at this point; this is managed by giving protamine and blood products. Temporary ventricular pacing wires are generally also placed, and, occasionally, atrial wires can also be placed. Typically, at least 2 chest tubes are placed to drain the mediastinum/left chest. Sternal closure is most often done with sternal wires, though other systems are sometimes used. Fascia, subcutaneous tissue, and skin is then closed. As you are closing, the nurse will connect the chest tubes to suction and look for blood accumulating in the tubing. This is referred to as “timing”. To pass timing, you will need to see that no blood is accumulating in the chest tubes after 5 minutes; this is done at least 3 times. This gives us a rudimentary assessment if bleeding is a concern before drapes are taken down and the patient is brought to the ICU.
You should stay with the patient as the patient is brought out of the OR and transferred to the ICU. As drips are disconnected/reconnected and the patient’s hemodynamic monitoring is transitioned, or as the patient is rolled/moved, patients can have significant hemodynamic changes and you should always be watching for these. Typically, it is a good idea to stay at the patient’s bedside in the ICU until all the monitors are hooked up, report has been given to the nurse and the ICU residents/attending, hemodynamics are stabilized, and you are satisfied that there isn’t major uncontrolled bleeding. If in doubt, notify the attending immediately.
A video outline of cardiopulmonary bypass can be found here.
Routine postoperative care
Postop cardiac surgery patients have a standard protocol that the nurses follow for routine care. This may not be appropriate in all patients; the attending will let you and the nurses know what he wants. Typically, if there is no significant bleeding over the next few hours postop, the pressors and inotropes will be slowly weaned off and the patient will be allowed to wake up, with the goal of extubating within 6 hours. Typically, on POD 1, the Swan-Ganz catheter is removed and the patient is ambulated. Beta blockers and diuretics are frequently begun. Aspirin, lovenox, and sometimes other anticoagulants are begun. Chest tubes are removed by the ICU nurses at the direction of the surgeon when the output is low (generally less than 200cc/day). By POD 2, central lines, foley, and chest tubes are generally out. Patients at this stage generally transfer to telemetry. The remainder of the postoperative course is working on pain control, ambulation, and medication adjustments for heart rate/blood pressure/diuretics/anticoagulation. The NPs on the floor will handle most of the routine orders and make arrangements for outpatient f/u, home health care services, etc. Typically, patients are ready for discharge home after uncomplicated cardiac surgery by POD 5.
Postoperative Complications
Generally speaking, you will not be called for the cardiac surgery patient that is doing well. The nurses and ICU residents will be calling you to help address problems. In dealing with any of these issues, if you have concerns or questions about what is the most appropriate treatment, contact the attending directly and ask. All of us will want to know early if there are postoperative issues with our patients. Some of the more common problems cardiac surgery patients encounter are listed below.
Bleeding/tamponade
As previously mentioned, there is always some degree of bleeding after heart surgery. Bleeding from coagulopathy can happen as clotting factors are consumed by the use of the cardiopulmonary bypass machine, heparin is given, or platelets don’t work due to medications the patient was on preoperatively. Obviously, not all bleeding is from coagulopathy, and evaluation in the OR to achieve adequate hemostasis is mandatory. Timing at the end of the case is useful to see if the bleeding is under control; if you are not making times, you should not leave the OR and you need to let the attending know. While 3x5min is a common method used, some attendings will use different metrics to assess for bleeding; they will let you know what they want. Once the patient is brought to the ICU, it is a good idea to record the level of the chest tube output (frequently there is a dump of blood as the patient is being jostled and moved). If there is a concern for bleeding in the ICU, make sure to keep the chest tubes patent by stripping the chest tubes; this is done by applying lotion or other lubrication to the soft part of the tubing and pulling it backwards, creating a suction in the chest tube and allowing clots to be pulled backwards. Keep an eye on the chest tube output at 15 minute intervals initially. Generally, output >100cc/hr is too much. Blood products, K centra, protamine, or Factor VII may all be given, but, if this persists, the patient may need to return to the OR.
In managing a bleeding patient with the chest closed in the ICU, you must be aware of the possibility of tamponade, even if the chest tubes are patent and working. Look for hypotension unresponsive to pressors, a reduction of cardiac output as measured by the Swan-Ganz catheter, and an equalization of the CVP and the PA diastolic pressure. To help make the diagnosis, a chest x-ray may be helpful to look for a widened mediastinum. You can also request either a bedside transthoracic echo (done by the cardiology fellow) or a transesophageal echo (done by cardiac anesthesia) to look for fluid around the heart and see if that fluid is collapsing the RV in diastole. If you are worried about tamponade in any patient, call the attending immediately.
There are extreme cases where there is tamponade in a patient in the ICU and there is no time to bring the patient to the OR. You should be discussing these situations with the attending, and you may be directed to open the chest in a patient in the ICU. This is only to be done at the explicit instruction of the CV surgery attending. There is a cart in the ICU that has the instruments you would need for this: a sterile drape to drape the chest, a scalpel to reopen the skin and cut the sutures for the subcutaneous and fascial closures, a heavy twister to partially untwist the sternal wires, a wire cutter to cut the sternal wires, and a sternal retractor to open the sternum. There is also suction tubing to connect to wall suction. Once the sternum is opened, the patient’s hemodynamics should immediately improve. If you see a bleeding source squirting at you, put your finger on it; otherwise, suction the blood and wait for the attending.
An informative video summary of this subject can be found here.
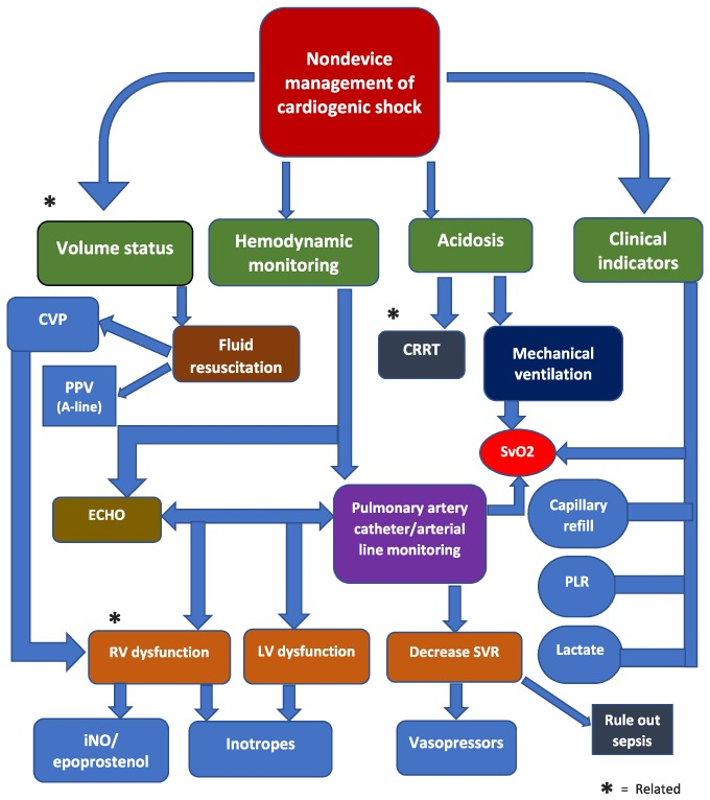
Cardiogenic shock
Outside of bleeding and tamponade, there are a number of reasons why a patient’s heart may not be working well after cardiac surgery. As the average patient has gotten older and sicker, we are frequently seeing patients with advanced heart disease and reduced ejection fraction that we offer heart surgery to. Prolonged cross clamp time, inadequate myocardial protection, pre-existing heart failure, and incomplete revascularization are some factors that may result in post-cardiotomy cardiogenic shock. This is manifested by low cardiac output in the absence of significant bleeding and without hypovolemia. The treatment is supportive with inotropes and pressors, and will be managed by the cardiac surgery attending. Sometimes, mechanical support with an intra-aortic balloon pump or ECMO may be needed. If you are called for a fresh postop heart that is not bleeding but has low cardiac output, you need to make an assessment of the patient’s volume status (based on CVP or PA pressures); if the patient is hypovolemic, give volume. If the CVP/PA pressures are elevated and the cardiac output is low, and the patient is not bleeding or in tamponade, then this is cardiogenic shock. The treatment is support with inotropes; contact the attending early with this situation. A useful algorithm is shown above.
Further information about cardiac physiology and hemodynamic monitoring can be found in this video.
Outside of bleeding and tamponade, there are a number of reasons why a patient’s heart may not be working well after cardiac surgery. As the average patient has gotten older and sicker, we are frequently seeing patients with advanced heart disease and reduced ejection fraction that we offer heart surgery to. Prolonged cross clamp time, inadequate myocardial protection, pre-existing heart failure, and incomplete revascularization are some factors that may result in post-cardiotomy cardiogenic shock. This is manifested by low cardiac output in the absence of significant bleeding and without hypovolemia. The treatment is supportive with inotropes and pressors, and will be managed by the cardiac surgery attending. Sometimes, mechanical support with an intra-aortic balloon pump or ECMO may be needed. If you are called for a fresh postop heart that is not bleeding but has low cardiac output, you need to make an assessment of the patient’s volume status (based on CVP or PA pressures); if the patient is hypovolemic, give volume. If the CVP/PA pressures are elevated and the cardiac output is low, and the patient is not bleeding or in tamponade, then this is cardiogenic shock. The treatment is support with inotropes; contact the attending early with this situation. A useful algorithm is shown above.
Further information about cardiac physiology and hemodynamic monitoring can be found in this video.
Major arrhythmias
In the OR, as the heart is being rewarmed and reperfused, it is not uncommon to have arrhythmias such as ventricular tachycardia, ventricular fibrillation, or torsades des pointes. These are usually transient and are treated by defibrillation with internal paddles and lidocaine and magnesium. In the ICU, it is uncommon to have major ventricular arrhythmias; it usually means there is some underlying problem such as an early graft failure or postop MI. If you are called to see a patient in ventricular tachycardia or ventricular fibrillation in the ICU, defibrillate the patient (per ACLS protocols) and then contact the attending.
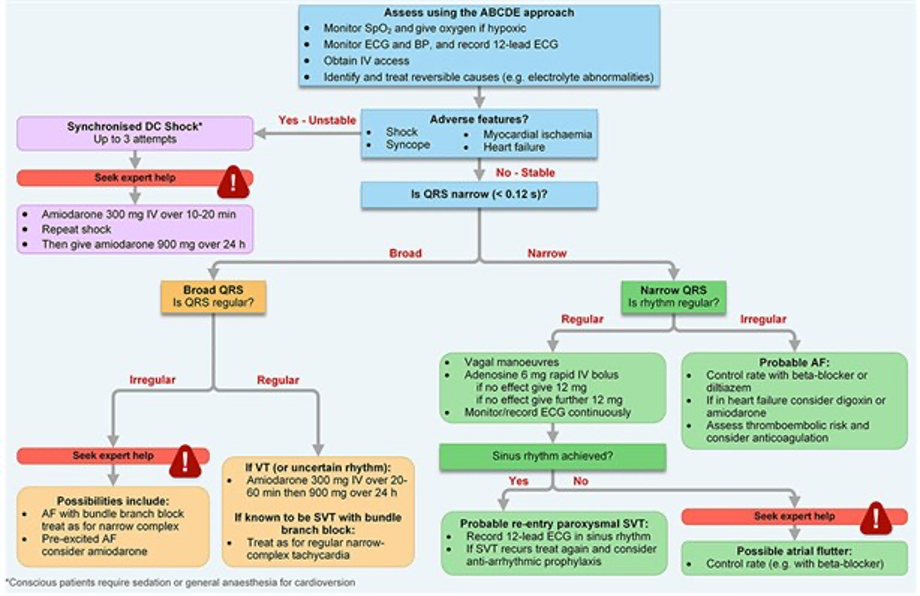
Atrial fibrillation is much more common than ventricular arrhythmias in postop cardiac surgery patients. It can occur any time in the postoperative period, but is most common to occur between POD 2-5, as the patient’s body mobilizes fluid during this period. For patients with hemodynamically unstable afib, per ACLS protocol, the treatment is synchronized cardioversion. For patients with uncontrolled afib who are not hypotensive, IV amiodarone is the preferred treatment. IV beta blockers or diltiazem are also commonly used. If the patient is on telemetry with rapid afib, you should consider transferring the patient back to the ICU if you have concerns about hypotension or he isn’t responding to initial therapy.
Bradyarrhythmias can also happen in postop cardiac patients. Generally, the patients have temporary epicardial ventricular pacing wires (typically pacing wires are removed just before discharge). If you are called for a patient having HR<50 and hypotension, a good first step is to get an EKG. Patients can have HR <50 while they sleep; this typically does not cause hypotension. Sinus bradycardia is typically benign and usually doesn’t cause too much hypotension; hold the patient’s beta blockers. For junctional rhythms, complete heart block, and any wide complex bradycardia, start ventricular pacing the patient at 80 beats/minute and see if the patient’s hemodynamics improve. Contact the attending if the patient is now requiring pacing where previously it wasn’t needed and consider transfer back to the ICU if the patient is on telemetry.
Stroke
Routine cardiac surgery has a 1-2% risk of stroke. This can be increased depending on the age of the patient, what procedure the patient had done, whether multiple cross clamps were needed, if the patient has carotid disease or atherosclerotic disease involving the aorta, if there was a prolonged cross clamp or need for circulatory arrest, if there was significant preoperative or intraoperative hypotension or hypoxia, if the patient has atrial fibrillation or LV thrombus, or if the patient had a prior history of CVA. Generally, we give patients 24 hours after sedation is held before we start investigating. Most postop CVAs are ischemic or embolic, but occasionally hemorrhagic strokes occur and they should be managed by consulting neurosurgery.
If you are called to see a patient who is POD 0-1 and wakes up with a specific neurologic finding, contact the CV attending. The stroke team should be contacted, but there is likely no other intervention that will be done, as patients are that stage are not candidates for thrombolytic therapy or mechanical thrombectomy. The exception to this is the thoracoabdominal aneurysm patient who develops sudden paralysis or loss of bladder/bowel continence. In these patients, make sure the spinal drain is open and working, keep their blood pressure elevated (MAP>80), and contact the CV attending immediately.
Dyspnea
If you are called about a patient in respiratory distress on telemetry, transfer the patient back to the ICU. Our threshold to re-intubate patients in respiratory distress is fairly low, as postop cardiac surgery patients generally do not do well with non-invasive ventilation for a prolonged period of time. If a patient is requiring >6L oxygen on telemetry, transfer the patient to the ICU.
Low urine output
In the early postoperative period, low urine output is either a sign of inadequate cardiac output (as would be seen on the swan), hypovolemia, or AKI. By POD 2-3, most patients have begun to mobilize the fluid they got during surgery. If they are having low urine output at this time, it is either due to AKI or not enough diuretic. Typically, we try to diurese patients such that they are negative 1-1.5L/day between POD 2-5. As with other surgical patients, you will need to make an assessment of the patient’s volume status, and then determine if fluids or additional diuretics are appropriate.
Altered mental status
Outside of acute CVAs, many older patients will experience some form of delirium, especially at night, that you may be called about. As in all patients that you are evaluating for altered mental status, you need to consider possible etiologies such as hypoglycemia or hypoxia or drug/alcohol withdrawal. You will need to consider what medications the patient may have recently received. We try to avoid using of benzodiazepines in our patients, and we avoid the use of sleep aids. For the acutely delirious patient who is fighting or trying to remove tubes, etc., Haldol is a useful drug.
Fever
Similar to other surgery patients, fever in cardiac surgery patients POD 0-2 is usually atelectasis, POD 2-4 is often a UTI, and POD 3-5 is often a surgical site infection or pneumonia. Patients can develop low grade fevers starting POD 2 from PPS (post-pericardiotomy syndrome), which is not infectious and thought to be related to inflammation of the pericardium after heart surgery. This is usually treated by anti-inflammatories and colchicine; steroids may also be used. We are especially cautious about fevers in patients with valve replacements or prosthetic grafts or VADS. Don’t hesitate to start broad spectrum antibiotics in these cases and send cultures.
Anemia/Thrombocytopenia
Blood loss after cardiac surgery is a common occurrence. For most patients, we do not transfuse unless the hemoglobin is <8g/dl. If an attending has a different hemoglobin goal, he will let you know. If the patient is actively bleeding in the early postoperative period, you may need to transfuse more aggressively.
Thrombocytopenia in the postoperative period can be caused by a number of factors. Consumptive thrombocytopenia from bleeding is one example. Another is heparin-induced thrombocytopenia, which is an immune-mediated response to heparin that results in platelet clumping/aggregation, which can cause ischemia to end arteries (black toes, tissue loss etc.) and low platelet counts. This is diagnosed by send a HIT panel and an SRA; the treatment is stopping all heparin products and starting anticoagulation with argatroban.
In non-bleeding patients, we don’t tend to transfuse platelets unless they are less than <20K. If a patient needs any kind of procedure, we like the platelet count to be at least 50K. If a patient is bleeding, try and keep platelets >100K.
Pericardial/pleural effusions
As you round on cardiac surgery patients, you may encounter patients after heart surgery that develop postop pleural or pericardial effusions. Pericardial effusions after heart surgery are usually related to pericarditis; if they are large or are thought to be causing hemodynamic compromise, they are drained either by pericardiocentesis or by doing a pericardial window. Pleural effusions are more common. If large or if they are felt to be the cause of a patient’s dyspnea, they can be drained either by thoracentesis or chest tube placement. You may be asked to participate in these procedures on the weekend; if you are unfamiliar with how to do these procedures the attending will guide you.
Wound infections
Historically, the most common wound infections in cardiac surgery patients were wound infections related to the harvest of the greater saphenous vein in the leg. This has been improved, but not eliminated, by the use of endoscopic vein harvest. These infections are treated like other soft tissue infections with antibiotics and surgical drainage as needed.
Sternal wound infections are much less common. If you are asked to see a patient with a possible sternal wound infection, look at the wound, looking for areas of erythema or drainage. Then, palpate the sternum in the manubrium and the body, using your thumb and index finger on the right and left sides of the sternum, and ask the patient to cough. Look for signs of sternal instability. Large volume drainage from the wound, sternal instability, severe pain, and fever/sweats/chills are potential signs of deep sternal wound infection (infection at or below the level of the sternum) and should be evaluated further by CT scan. These may require surgical treatment in the OR. Superficial sternal wound infections can be managed with antibiotics and I&D as indicated.
Leg swelling
Leg swelling after harvesting the greater saphenous vein is common. The greater saphenous vein is generally responsible for 10% of the venous return of the leg; taking it necessarily reduces the venous return of the leg and may cause unilateral leg swelling. If the patient has severe leg swelling, this is generally treated with leg elevation and compression with ace wraps or compression stockings. DVT is also in the differential and may be investigated by ultrasound. Bilateral leg swelling is usually an indication of congestive heart failure or volume overload and is treated by diuretics.
Final remarks
As with any primer, this is not intended to be an all-encompassing review of cardiac surgery. This is intended as an introduction to cardiac surgery and a reference to dealing with common problems. In dealing with all the problems you may encounter with cardiac surgery patients, your attending CV surgeon is your best resource, and you should not hesitate to contact the attending CV surgeon if problems arise. Other team members, such as the ICU attending/residents, nurses, anesthesiologists, perfusionists, etc. are all there to help you, and you should solicit their advice as you learn. Familiarity with ACLS and common ICU management is helpful (the ICU book by Marino is a good starting point). Regarding specific procedures, there is a lot of good information on the internet, including full videos of various procedures, which you can look up as you prepare for a case.
Additional informational videos on various subjects related to cardiac surgery can be found here.
We hope you will enjoy your experience on cardiac surgery, that you will learn a lot, and that you will gain a new appreciation for the work we do. Good luck!
